 Shoulder bursitis is also known as shoulder impingement or rotator cuff tendonitis. It can be caused by injury, overuse, or a bone spur in the shoulder.
Shoulder bursitis is also known as shoulder impingement or rotator cuff tendonitis. It can be caused by injury, overuse, or a bone spur in the shoulder.
Bursitis is an inflammation of a bursa, which is a small fluid-filled sac found around a joint. It acts as a cushion between moving parts in the joint to stop muscles, bones, and tendons from rubbing together.
When your shoulder bursa gets irritated, it becomes inflamed and develops scar tissue. This causes inflammation of the muscles and tendons. Their role is to move the shoulder, and the inflammation can cause pain and loss of movement in the shoulder.
A common cause of shoulder bursitis is overuse of the shoulder joint, especially if that activity is performed repetitively or overhead. If you are doing sport or work that involves repetitive movements it can put stress on your shoulder joint. It is also important to be careful with exercises that require repetitive movements.
 You may come across different terms for what is commonly called shoulder bursitis. The terms ‘shoulder impingement’, ‘rotator cuff tendonitis’, and ‘subacromial bursitis’ refer to a spectrum of the same condition.
You may come across different terms for what is commonly called shoulder bursitis. The terms ‘shoulder impingement’, ‘rotator cuff tendonitis’, and ‘subacromial bursitis’ refer to a spectrum of the same condition.
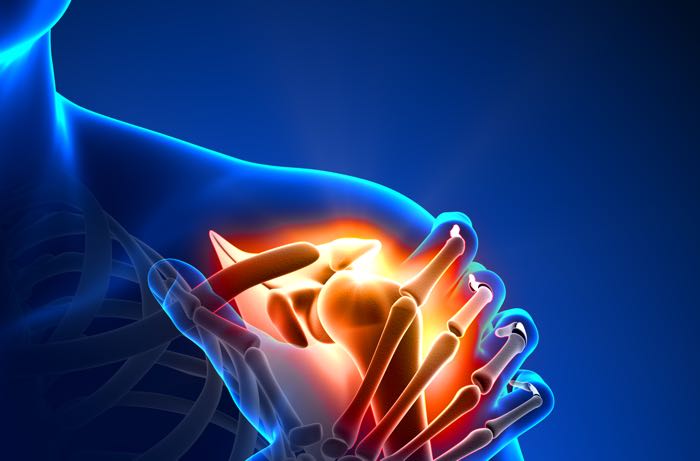
Impingement occurs when the tendons of the rotator cuff rub against the undersurface of the acromion bone when you lift the arm. The acromion impacts against the rotator cuff tendons, hence the term ‘impingement’.
Rotator cuff tendonitis occurs when the tendons rubbing against the bone becoming inflamed.
Subacromial bursitis is inflammation of the bursa which sits between the bone and the tendons. The bursa is a normal structure allowing the tendons to move freely against the bone. Shoulder bursitis and rotator cuff tendonitis cause pain.
In younger patients, impingement often results from injury or overuse. Irritation of the tendon causes it to swell and the more it swells the more it rubs against the acromion bone. More rubbing causes more swelling and the cycle continues.
In older patients, impingement and tendonitis are more likely to occur when a subacromial spur forms. The spur is an overgrowth of bone which impacts on the rotator cuff tendons when the arm is lifted. This can eventually lead to a rotator cuff tear. keeping your arm by your side.
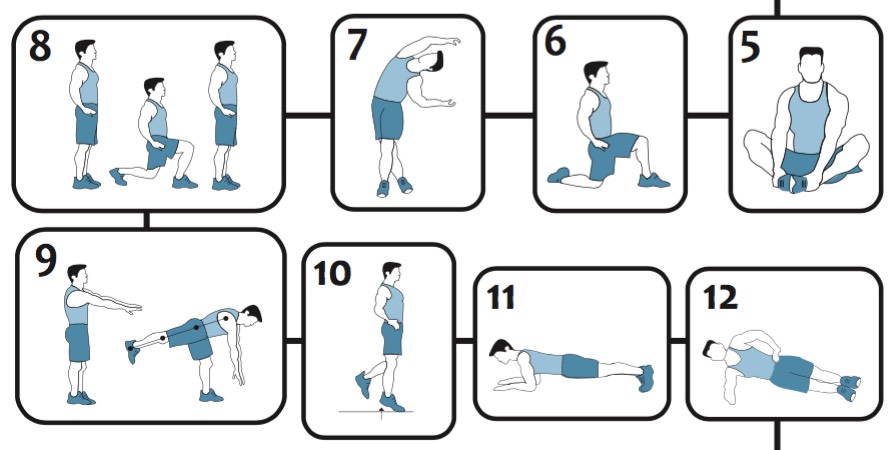 In the field of shoulder and knee reconstruction, successful outcomes from an operation are 50% surgery and 50% rehabilitation.
In the field of shoulder and knee reconstruction, successful outcomes from an operation are 50% surgery and 50% rehabilitation.
You could say the surgery is the easy bit, the rehabilitation is all hard slog. Dr Colvin’s CO.RE exercise programs are just that, a core plan for your successful recovery.